Download this article and more from our free toolbox!
By: Sean M. Scott
In the restoration industry today, a lot of attention is given to the testing and abatement of microscopic hazardous materials. These include asbestos, lead, mold, bacteria, bloodborne pathogens, and all sorts of bio-hazards fall into this category. If these contaminants are disturbed, treated, or handled improperly, all of them can cause property damage and serious harm to the health and welfare of those living or working in or near the areas where they’re present. However, there are other hazardous toxins that commonly present themselves in restoration projects, that seem to go unnoticed. These are the toxic smoke particulates and volatile organic compounds (VOC’s) created during structure fires.

Photo courtesy of Mark Doyle
When a building is abated from asbestos, lead, or mold, special care is given to be sure every microscopic fiber, spore, and bacteria is removed. This is done through extensive cleaning, HEPA vacuuming, chemical applications, negative air, and other procedures.
Once the remediation is completed, an independent environmental testing laboratory or industrial hygienist provides an air clearance test to certify that the abatement or remediation process was successful. Upon receipt of the clearance, people can then reenter the remediated area, rooms, or building. However, when the structural repairs are completed after a fire, an air clearance test is rarely ever performed. How then can consumers be assured or restoration companies guarantee that the billions of toxic particulates and VOC’s generated by the fire have been removed? Is there cause for concern or is a simple “sniff” test or wiping a surface with a Chem- sponge sufficient? Why is it so common to hear customers complain of smelling reoccurring smoke odor long after the restoration is completed? What measures are being taken to protect workers and their families from toxic ultra-fine particulate matter or VOC’s?
In the following pages, we will be taking a close look at this issue to raise awareness of a segment in the fire restoration industry that has been long overlooked and, in most cases, disregarded entirely.
WHAT IS SMOKE?

Smoke is a complex mixture of toxic gases and particles, which are generated from the vast array of materials that burn during a fire. A typical structure fire may generate literally tens of thousands of toxic chemicals and gasses. Research on cigarette smoke alone has identified over 7,000 chemicals, with 70 identified as cancer causing, even with brief exposure.(1) Studies haven’t even scratched the surface to determine all the potentially adverse health effects that may result from exposure to the chemicals released from the combustion of the multitude of products in a structure fire. These include plastics, foams, textiles, carpets, wood products (treated lumber, plywood, flooring), synthetic fabrics, wool, electronics, furniture, household chemicals, and the list goes on. One of the biggest health threats from smoke is from fine and ultra-fine particles. These microscopic particles can penetrate deep into the lungs and can cause a range of health problems, from burning eyes and a runny nose to aggravated chronic heart and lung diseases and cancer. Exposure to particle pollution is even linked to premature death.(2) Exposure to smoke toxins can be far more hazardous to human health than mold, asbestos, lead, or other contaminants. Respiratory ailments, cardiac hazards, and cancers connected with exposures to an environment affected by a fire are far greater than those from the past, mainly because the materials used today to manufacture our products and their chemical composition have changed dramatically.
THE HIDDEN HAZARDS OF FIRE SOOT (3)
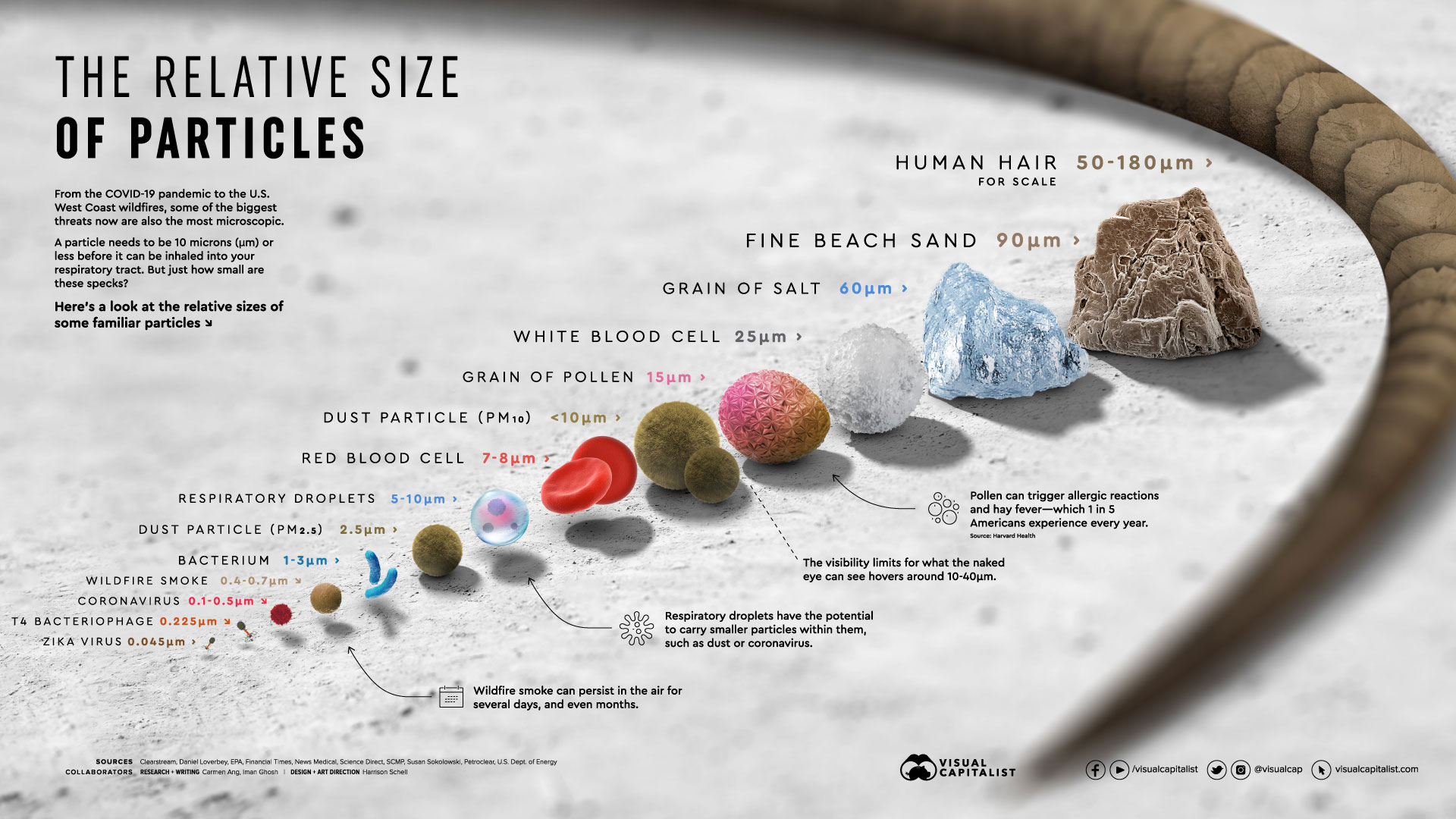
Click image for larger view
Smoke is the result of incomplete combustion, which produces tiny particles of carbon in the air. When deposited, these particulates are identified as soot. Put simply, the particle size of smoke residue on a surface can present a respiratory hazard. The particle size of soot is approximately 2.5 microns or less, a size that is associated with deep lung penetration. Particles that are approximately 10 microns or larger get trapped in the upper respiratory tract. Particles that are 5 microns or smaller can make it down to the lower lung where the gas exchange occurs in the alveoli. To offer some perspective on the size of these particles, red blood cells are approximately 7 microns in size. The dust you see flying in the light coming through a sun lit window are about 40 microns in size. Airborne soot is too small to be seen with the naked eye and can easily be inhaled. When you inhale, you take in air and any particles that are in the air. The breath, along with the particles, travel through your respiratory system to your lungs. Along the way, particles can become caught in your nasal or sinus system, causing discomfort or potential health problems.
As a fire dies down, the smoke will disperse leaving behind a residue of quickly cooling particles which is generally referred to as soot. Typically, soot is representative of what has burned, but may include byproducts that at first seem unrelated to the original material.
For example, hydrogen cyanide is a byproduct of burning wool. When wood burns it can produce manganese, benzene, and dioxins. As many products as there are in the world, there are an equal number of byproducts produced in a fire and many are known carcinogens or extremely hazardous when inhaled or absorbed by the skin.
 A common house fire results in the burning of a wide variety of materials, from wood and paper to plastics and other synthetic items. Breathing the tiny particles can cause coronary heart disease, asthma, bronchitis, and many other respiratory illnesses.
A common house fire results in the burning of a wide variety of materials, from wood and paper to plastics and other synthetic items. Breathing the tiny particles can cause coronary heart disease, asthma, bronchitis, and many other respiratory illnesses.
Research has also shown that many premature deaths are directly related to soot in the environment. Particle exposure leads to around 20,000 premature deaths in America each year. Many of these deaths were caused by soot-related diseases. Data also shows that soot annually causes almost 300,000 asthma attacks and 2 million lost workdays due to respiratory problems.(4)
While we would not expect most VOC’s to survive a fire and still be present on the soot, there may be metals present as well as some chlorinated compounds. The Phoenix Fire Department examined this phenomenon during a study focused on firefighter exposures after a fire was extinguished and their findings indicated that some chlorinated products such as dioxin become attached to airborne particulate matter. This is an important study because it points to the fact that exposure to airborne vapors and residues after a fire are much more complex than our current understanding allows. However, the important point is that soot may be more than just a particulate hazard; it can potentially carry other chemical residues that are potentially harmful to the respiratory system.
TOXIC CHEMICALS AND GASES
The toxic mixture of chemicals and gasses contained in fire smoke is comprised primarily of carbon monoxide, carbon dioxide, hydrogen cyanide, ammonia, hydrogen chloride, sulfur dioxide, hydrogen sulfide, acids, and oxides of nitrogen. Other toxins may include dioxins, furans, polychlorinated biphenyl (PCB’s) acetylene, methyl mercaptan, ammonia, nitric oxide, carbon disulfide, creosote, nitrogen dioxide, dimethyl sulfide, phosphine, ethylene, benzene, methylene chloride, lead, chromium, and other metals, trichloroethylene, toluene, trichlorophenol, fluorine, acrolein, mercury, formaldehyde, benzaldehyde, sulfuric acid, hydrochloric acid, arsenic, chromate, phenol, styrene, polycyclic aromatic hydrocarbons (PAH’s), etc.
 Chlorine gas was the first lethal chemical to be used in World War I, resulting in thousands of casualties. Then later phosgene and diphosgene were used. Hydrogen cyanide was also produced, but its physical properties were found to be unsuitable for use as an effective chemical warfare agent. (Hydrogen cyanide and phosgene are both commonly found in structure fire smoke) Phosgene was first used as a Chemical Weapon by the Germans, but was later used by the French, Americans, and British. Initial deployment of the gas was by the Germans at Ypres Salient on December 19, 1915 when they released around 4000 cylinders of phosgene combined with Chlorine against the British. Phosgene was responsible for the majority of deaths that resulted from chemical warfare.(5)
Chlorine gas was the first lethal chemical to be used in World War I, resulting in thousands of casualties. Then later phosgene and diphosgene were used. Hydrogen cyanide was also produced, but its physical properties were found to be unsuitable for use as an effective chemical warfare agent. (Hydrogen cyanide and phosgene are both commonly found in structure fire smoke) Phosgene was first used as a Chemical Weapon by the Germans, but was later used by the French, Americans, and British. Initial deployment of the gas was by the Germans at Ypres Salient on December 19, 1915 when they released around 4000 cylinders of phosgene combined with Chlorine against the British. Phosgene was responsible for the majority of deaths that resulted from chemical warfare.(5)
To illustrate the types of chemicals found in structure fires, here is a list of some of the most common toxic chemicals and gases and their effects on human health:
Benzene
https://www.cancer.org/cancer/cancer-causes/benzene.html
The International Agency for Research on Cancer classifies benzene as carcinogenic to humans, based on sufficient evidence that benzene causes acute myeloid leukemia. Benzene exposure has been linked with acute lymphocytic leukemia, chronic lymphocytic leukemia, multiple myeloma, and non-Hodgkin lymphoma.
Arsenic
https://globalhealing.com/natural-health/health-dangers-arsenic-toxicity/
Arsenic is an element that is extremely toxic to human health. Arsenic poisoning occurs when someone is exposed to arsenic, typically by unknowingly ingesting it. Poisoning can occur by inhalation or through dermal absorption.
Sulfur Dioxide
https://www.atsdr.cdc.gov/phs/phs.asp?id=251&tid=46
Sulphur Dioxide reacts with humidity and forms sulphuric and sulphurous aerosol acid. It causes breathing difficulty, airways inflammation, psychic alterations, pulmonary edema, heart failure, and circulatory collapse. Sulphur dioxide is also associated with asthma, chronic bronchitis, and mortality increase in the elderly and infants.
Hydrogen Cyanide
https://www.atsdr.cdc.gov/MMG/MMG.asp?id=1141&tid=249
Breathing small amounts of hydrogen cyanide may cause headache, dizziness, weakness, nausea, and vomiting. Larger amounts may cause irregular heartbeats, seizures, fainting, and rapid death.
Hydrogen Sulfide
https://www.atsdr.cdc.gov/MMG/MMG.asp?id=385&tid=67
Symptoms of acute exposure include nausea, headaches, delirium, disturbed equilibrium, tremors, convulsions, and skin and eye irritation. Inhalation of high concentrations of hydrogen sulfide can produce rapid unconsciousness and death.
Formaldehyde
https://www.cancer.org/cancer/cancer-causes/formaldehyde.html
The International Agency for Research on Cancer has concluded that formaldehyde is carcinogenic to humans, based on higher risks of nasopharyngeal cancer and leukemia.
Phosgene
https://emergency.cdc.gov/agent/phosgene/basics/facts.asp
During or immediately after exposure to dangerous concentrations of phosgene, the following signs and symptoms may develop: Coughing, burning sensation in the throat and eyes, watery eyes, blurred vision, difficulty breathing or shortness of breath, nausea and vomiting. Skin contact can result in lesions similar to those from frostbite or burns. Exposure to phosgene may cause delayed effects that may not manifest for up to 48 hours after exposure, even if the person feels better or appears well following removal from exposure. Therefore, people who have been exposed to phosgene should be monitored for 48 hours afterward. Delayed effects that can appear for up to 48 hours include the following: Difficulty breathing, coughing up white to pink-tinged fluid (a sign of pulmonary edema) low blood pressure, and heart failure.
Mercury
https://www.atsdr.cdc.gov/toxfaqs/TF.asp?id=113&tid=24#bookmark05
Methylmercury and metallic mercury vapors are more harmful than other forms, because more mercury in these forms reaches the brain. Exposure to mercury can permanently damage the brain, kidneys, and developing fetus. Effects on brain functioning may result in irritability, shyness, tremors, changes in vision or hearing, and memory problems. Very young children are more sensitive to mercury than adults. Mercury in a mother’s body passes to the fetus and may accumulate there. It can also pass to a nursing infant through breast milk. Mercury’s harmful effects that may be passed from the mother to the fetus include brain damage, mental retardation, incoordination, blindness, seizures, and inability to speak. Children poisoned by mercury may develop problems of their nervous and digestive systems, and kidney damage.
Styrene
https://www.osha.gov/SLTC/styrene/hazards.html
Chronic exposure affects the central nervous system showing symptoms such as depression, headache, fatigue, weakness, and may cause minor effects on kidney function.
Hydrogen Chloride
https://www.atsdr.cdc.gov/toxfaqs/tf.asp?id=759&tid=147
Hydrogen chloride is irritating and corrosive to any tissue it contacts. Brief exposure to low levels causes throat irritation. Exposure to higher levels can result in rapid breathing, narrowing of the bronchioles, blue coloring of the skin, accumulation of fluid in the lungs, and even death. Exposure to even higher levels can cause swelling and spasm of the throat and suffocation. Some people may develop an inflammatory reaction to hydrogen chloride. This condition is called reactive airways dysfunction syndrome (RADS), a type of asthma caused by some irritating or corrosive substances.
Phenol
https://www.atsdr.cdc.gov/mmg/mmg.asp?id=144&tid=27
Exposure to phenol by any route can produce systemic poisoning. Phenol is corrosive and causes chemical burns at the contact site. Coma and seizures can occur within minutes or may be delayed up to 18 hours after exposure. Other symptoms include nausea, vomiting, diarrhea, methemoglobinemia, hemolytic anemia, profuse sweating, hypotension, arrhythmia, pulmonary edema, and tachycardia. As a corrosive substance, phenol denatures proteins and generally acts as a protoplasmic poison. Phenol may also cause peripheral nerve damage. Systemic poisoning can occur after inhalation, skin contact, eye contact, or ingestion. Damage to the nervous system is the primary cause of death from phenol poisoning.
Acrolein
https://www.ncbi.nlm.nih.gov/pubmed/19028774
Acrolein vapor may cause eye, nasal and respiratory tract irritations in low level exposure. A decrease in breathing rate was reported by volunteers acutely exposed to 0.3A ppm of acrolein.
Methyl Mercaptan
https://www.atsdr.cdc.gov/MMG/MMG.asp?id=221&tid=40
Methyl mercaptan is a central nervous system depressant that acts on the respiratory center to produce death by respiratory paralysis. Individuals with pre-existing respiratory, cardiac, nervous system, or liver impairment may be more susceptible to exposure to methyl mercaptan.
Toluene
https://www.atsdr.cdc.gov/MMG/MMG.asp?id=157&tid=29
Toluene is irritating to the skin, eyes, and respiratory tract. It can cause systemic toxicity by ingestion or inhalation and is slowly absorbed through the skin. The most common route of exposure is via inhalation. Symptoms of toluene poisoning include central nervous system effects (headache, dizziness, ataxia, drowsiness, euphoria, hallucinations, tremors, seizures, and coma), ventricular arrythmias, chemical pneumonitis, respiratory depression, nausea, vomiting, and electrolyte imbalances. The mechanism by which toluene produces systemic toxicity is not known. Toluene crosses the placenta and is excreted in breast milk.
Trichloroethylene
https://www.atsdr.cdc.gov/phs/phs.asp?id=171&tid=30
People who are overexposed to moderate amounts of trichloroethylene may experience headaches, dizziness, and sleepiness; large amounts of trichloroethylene may cause coma and even death. Some people who breathe high levels of trichloroethylene may develop damage to some of the nerves in the face. Other effects seen in people exposed to high levels of trichloroethylene include evidence of nervous system effects related to hearing, seeing, and balance, changes in the rhythm of the heartbeat, liver damage, and evidence of kidney damage. Relatively short-term exposure of animals to trichloroethylene resulted in harmful effects on the nervous system, liver, respiratory system, kidneys, blood, immune system, heart, and body weight.
Polycyclic Aromatic Hydrocarbons
https://www.atsdr.cdc.gov/csem/csem.asp?csem=13&po=11
Increased incidences of lung, skin, and bladder cancers are associated with occupational exposure to PAHs. Epidemiologic reports of PAH- exposed workers have noted increased incidences of skin, lung, bladder, and gastrointestinal cancers. These reports, however, provide only qualitative evidence of the carcinogenic potential of PAHs in humans because of the presence of multiple PAH compounds and other suspected carcinogens.
For more detailed information on smoke particulate pollution and their effects on human health visit:
https://woodsmokepollution.org/references.html#particulate-references
DIOXINS
Dioxins are extremely toxic environmental pollutants known to science as persistent organic pollutants or (POPs).
Dioxins, especially 2,3,7,8-tetrachlorodibenzo-p- dioxin (TCDD) has been called the most toxic man- made compound on Earth.(6) Scientists say it is exceeded in toxicity only by radioactive waste.(7) Certain dioxin-like polychlorinated biphenyls (PCBs) with similar toxic properties are also included under the term dioxins.(8) A characterization by the National Institute of Standards and Technology of cancer causing potential evaluated dioxin as over 10,000 times more potent than the next highest chemical (diethanol amine), half a million times more than arsenic and a million or more times greater than all others. (9) TCDD has also been extensively studied for health effects linked to its presence as an ingredient in the herbicide Agent Orange, which was used as a defoliant during the Vietnam War.(10)
Burning of waste materials, such as in backyard burn barrels, creates higher levels of dioxins than industrial incinerators and is particularly dangerous because it releases pollutants at ground level where they are more readily inhaled or incorporated into the food chain. In comparison, the sheer volume of household products and building materials that combust in a typical structure fire can produce the equivalent of literally hundreds or even thousands of burn barrels.
Dioxins are formed when products containing carbon and chlorine are burned, such as plastics containing polyvinyl chloride (PVC). Even very small amounts of chlorine can produce dioxins.(11) During a structure fire, dioxins attach themselves to particles of soot and dust, where they spread efficiently into the air as the hot gases rise.
When a fire is extinguished, and the air begins to cool, the dioxin laden particles settle and become part of the soot, ash, and particulate matter. Burning 1 kilogram of wood can produce as much as 160 micrograms of total dioxins.
This result was obtained in a scientific experiment where various specimens of wood were burned in different stoves and analyzed by well-designed and documented procedures.
Highly chlorinated dioxins were present and the major components. In the soot from a series of experiments, their total content ranged from 10 to 167 mg/kg of fuel. The total yields of TCDD’s ranged from 0.1 to 7.8 mg/kg of fuel.” (12)
EFFECTS ON HUMAN HEALTH
 Short-term exposure of humans to high levels of dioxins may result in skin lesions, such as chloracne, similar to that shown on this child’s face, patchy darkening of the skin, and altered liver function. Long-term exposure is linked to impairment of the immune system, the developing nervous system, the endocrine system and reproductive functions.(13)
Short-term exposure of humans to high levels of dioxins may result in skin lesions, such as chloracne, similar to that shown on this child’s face, patchy darkening of the skin, and altered liver function. Long-term exposure is linked to impairment of the immune system, the developing nervous system, the endocrine system and reproductive functions.(13)
Other adverse health effects may include cardiovascular disease, diabetes, cancer, porphyria, endometriosis, early menopause, reduced testosterone and thyroid hormones, altered immunologic response, skin, tooth, and nail abnormalities, altered growth factor signaling, and altered metabolism.(14)
Dioxin, even in picograms (parts per trillion) is associated with severe health damage that can shorten the lives of people exposed to it, and potentially that of their offspring and future generations.
Dioxin is chemically stable and retained in human fatty tissue, where it alters the complex cellular and chemical balances involved in bodily functioning and reproductive processes. The genetic effects may skip a generation and reappear in third or subsequent generations. (15)
Diseases which have been linked to dioxin seem endless. Ingesting dioxin can also result in congenital malformations, spontaneous abortions, and a slow wasting syndrome followed by death similar to the AIDS syndrome. Dioxin is strongly suspected of contributing to pathology of the urinary and hematological systems, growths in the colon, gall bladder complications, multiple myeloma, and lung, larynx and prostate cancer.
According to researcher Joe Thornton, “Dioxin’s health effects include endocrine disruption, reproductive impairment, infertility, birth defects, lowered sperm counts, impaired neurological development, damage to the kidneys, and metabolic dysfunction…There is no evidence that there is a safe level of dioxin exposure below which none of these effects will occur…”
Many toxic chemicals are linked with a specific illness, such as lead and brain damage or asbestos and mesothelioma. Others are linked with several illnesses. Dioxin is tied to such a very large number of diseases because it is a cancer-enhancer. Dioxins intensify cancers which other toxics begin.
As Barry Commoner explains, “…dioxin greatly enhances the activity of the enzyme system that converts most environmental carcinogens into active agents. Apparently, dioxin can so powerfully stimulate the enzyme as to sharply increase the activity of the small amounts of carcinogens present in food, water, and air and thereby intensify their effect on tumor incidence. In effect, dioxin influences tumor production by enhancing the activity of carcinogens…”
This is why dioxin has totally different effects on different people. If a group of workers has already been exposed to chemicals which cause Hodgkin’s disease, dioxin will speed up the process and research will show that they have an increased rate of Hodgkin’s disease. If a community has been exposed to chemicals which cause leukemia, dioxin will increase the rate of leukemia. If chlorine is present when benzene is burned (and there is plenty of chlorine in plastics), hydrogen atoms can be released and chlorine atoms can replace them. The result are poly-chlorinated biphenyls, knows as PCBs. The presence of chlorine makes dioxins extremely stable compounds. They do not break down as easily as enzymes do. The human body tends to store dioxin in fatty tissue and when people take in dioxin through food or air, it ends up inside of their cells. (16)
Dioxins, furans, and PCB’s are three highly toxic chemicals identified by the EPA and the Stockholm Convention as members of the original “Dirty Dozen”, toxic chemicals that adversely affect human health and the environment. They can be transported by wind and water over long distances and can remain in the environment for centuries. They are all commonly found in structure fire smoke, VOC’s, and particulates.
Due to their high physical, chemical and biological stability, dioxins degrade very slowly by means of photolysis, (the decomposition or separation of molecules by the action of light), volatilization and biodegradation.
Photolysis is considered to be the most important degradation mechanism of gas phase dioxins in the atmosphere; however, laboratory evidence [Kwok et al 1995] indicates that when dioxins are associated with particles, photodegradation is reduced to insignificant levels and, therefore, is too slow to provide considerable protection to the environment. The POP group consists of two subgroups including both the polycyclic aromatic hydrocarbons and some halogenated hydrocarbons. In addition to dioxins and furans, the POP group includes many organochlorine insecticides such as dieldrin, DDT, toxaphene, chlordane, hexachlorobenzene, aldrin, endrin, heptachlor, toxaphene, mirex and several industrial chemical products or by-products including polychlorinated biphenyls (PCBs). The chlorinated compounds are generally the most persistent of all the halogenated hydrocarbons.
Because of the extremely high toxic potency of dioxins, the environment must be effectively monitored for even very low quantities.(17)
TOXICOKINETICS AND MECHANISM OF TOXICITY(18)
Toxic combustion products are classified as simple asphyxiants, irritant toxins, and chemical asphyxiants.
Simple asphyxiants are space occupying and fill enclosed spaces at the expense of oxygen. In addition to this effect, combustion uses oxygen and creates an oxygen-deprived environment.
 Irritant toxins are chemically reactive substances. They produce local effects on the tissue or the respiratory tract. Ammonia is produced by burning wool, silk, nylon, and synthetic resins. Ammonia has high water solubility and dissolves in moist membranes of the upper respiratory tract, resulting in nasopharyngeal, laryngeal, and tracheal inflammation. Acrolein is lipid soluble and penetrates cell membranes. It denatures nucleic acid and intracellular proteins and results in cell death. Acrolein is a very common irritant gas generated by combustion. Sulfur dioxide is found in more than 50% of smoke from fires. Sulfur dioxide reacts with the moist respiratory membrane mucosa, producing the potent caustic, sulfurous acid. PVC is ubiquitous in all sorts of building materials and household products. Structure fires where PVC has burned will have significant levels of dioxins in the soot, smoke, and ash.
Irritant toxins are chemically reactive substances. They produce local effects on the tissue or the respiratory tract. Ammonia is produced by burning wool, silk, nylon, and synthetic resins. Ammonia has high water solubility and dissolves in moist membranes of the upper respiratory tract, resulting in nasopharyngeal, laryngeal, and tracheal inflammation. Acrolein is lipid soluble and penetrates cell membranes. It denatures nucleic acid and intracellular proteins and results in cell death. Acrolein is a very common irritant gas generated by combustion. Sulfur dioxide is found in more than 50% of smoke from fires. Sulfur dioxide reacts with the moist respiratory membrane mucosa, producing the potent caustic, sulfurous acid. PVC is ubiquitous in all sorts of building materials and household products. Structure fires where PVC has burned will have significant levels of dioxins in the soot, smoke, and ash.
Materials and common household products made with PVC, include but are not limited to: Vinyl siding, vinyl window frames, electrical wire/cable insulation, lighting lenses, gutters, plumbing pipes, ductwork for HVAC systems, vinyl window shutters and mini-blinds, carpet and floor coverings, food and chemical containers, furniture, clothing, strollers, car seats, baby formula bottles, toys, etc.
The resultant combustion products, phosgene, chlorine, and hydrogen chloride are produced in many residential fires. Together with water in the mucosa, chlorine produces hydrogen chloride free oxygen radicals and is very damaging to tissue.
Phosgene descends and produces more delayed alveolar injuries. Isocyanates are produced from burning and smoldering upholstery, and intense irritation of both upper and lower respiratory tissue results. Soot has not only carbon, but also aldehydes, acids, and reactive radicals that adhere to its surface. Inhalation of soot and associated aerosols heightens the effect of other irritant toxins. Soot binds with respiratory mucosal surfaces, allowing other irritant chemicals to adhere and react with adjacent tissue. The penetrance and deposition of these particles within the respiratory tract depend on size. Small particles (1 to 3 microns) reach the alveoli. Lung injury decreases when smoke is filtered to remove particulate matter. Sulfur dioxide shows a high propensity to adhere to soot. In addition, polyvinyl chloride combustion produces a large amount of soot-containing smoke coated with its particular combustion products such as phosgene, chloride, and hydrogen chloride. Irritant gases, acids, and other combustion products can also adhere to aerosol droplets.
The most important determining factor in predicting the level of respiratory injury is the water solubility of the toxin. Water-soluble chemicals injure the mucosa of upper respiratory airways by releasing the mediators of inflammation and deleterious free radicals. This type of inflammation increases microvascular membrane permeability and results in a net influx of fluid from intravascular spaces into the upper respiratory tissue. The underlying tissue of the supraglottic larynx may become terrifically swollen and edematous. This edematous reaction can result in minutes to hours post exposure, continue to progress, and close off upper airways completely.
Low water-soluble molecules react with the lung parenchyma. They react more slowly and produce delayed toxic effects. Concentration of the toxic element inhaled, particle size, duration of exposure, respiratory rate, absence of protective reflexes, preexisting disease, and age also contribute to the level and degree of respiratory injury in addition to the water solubility of toxins.
An intense inflammatory reaction develops secondary to the initial injury to respiratory mucosal cells by toxic combustion products. Inhaled soot and toxic gases generate increased airway resistance caused by inspissated secretions, increased mucosal airway edema, and associated bronchospasm. Damaged mucosal cells stimulate copious exudates rich in protein, inflammatory cells, and necrotic debris. If this reaction continues, mucosal sloughing ensues. The degenerative exudates, bronchorrhea, and extensive sloughing produce casts of the airways. In animal victims of smoke inhalation, these casts increase airway resistance by blocking major airways and prevent oxygen passage to the alveoli. Increased vascular permeability of respiratory tissue contributes to airway blockage.
Nitrogen-containing products, such as wool, silk, nylon, plastics, paper, rubber, pyroxylin, polyurethanes, and polyacrylonitriles, all produce cyanide at combustion.
 Cyanide has been detected in samples from many other types of fires as well. Other combustion products can cause systemic and local toxicity. Metal oxides, hydrogen fluoride, hydrogen bromide, and various types of hydrocarbons can all be retrieved from toxic smoke.
Cyanide has been detected in samples from many other types of fires as well. Other combustion products can cause systemic and local toxicity. Metal oxides, hydrogen fluoride, hydrogen bromide, and various types of hydrocarbons can all be retrieved from toxic smoke.
Benzene can be detected in the smoke of plastic and petroleum fires. Antimony, cadmium, chromium, cobalt, iron, lead, and zinc have all been recovered from smoke samples during fires. In fact, the entire spectrum of potentially toxic combustion products from fires is limitless. In addition, short-term exposure to fine particulates has been associated with triggering heart attacks, particularly among people with pre-existing heart disease.
FIREFIGHTER EXPOSURE TO SMOKE PARTICULATES (19)
 Underwriters Laboratories in collaboration with the Chicago Fire Department and the University of Cincinnati College of Medicine, recently completed a sixteen-month study on the smoke and gas exposure firefighters confront during firefighting operations and subsequent contact exposure resulting from residual contamination of personal protective equipment.
Underwriters Laboratories in collaboration with the Chicago Fire Department and the University of Cincinnati College of Medicine, recently completed a sixteen-month study on the smoke and gas exposure firefighters confront during firefighting operations and subsequent contact exposure resulting from residual contamination of personal protective equipment.
This study investigated and analyzed the combustion gases and particulates generated from three scales of fires: residential structure and automobile fires, simulated real-scale fire tests, and material based small-scale fire tests. Material-level tests were conducted to investigate the combustion of forty-three commonly used residential building construction materials, residential room contents and furnishings, and automobile components under consistent, well- controlled radiant heating conditions. In these tests, material-based combustion properties including weight loss rate, heat and smoke release rates, smoke particle size and count distribution, and effluent gas and smoke composition were characterized for a variety of natural, synthetic, and multi-component materials under flaming. The results from these tests were used to assess the smoke contribution of individual materials.
Nine real-scale fire tests representing individual room fires, an attic fire, deck and automobile fires were conducted at UL’s large-scale fire test laboratory to collect and analyze the gas effluents, smoke particulates, and condensed residues produced during fire growth, suppression and overhaul under controlled, reproducible laboratory conditions.
KEY FINDINGS
- The type and quantity of combustion products (smoke particles and gases) generated depended on the chemistry and physical form of the materials being burned.
- The most prolific smoke production was observed for styrene-based materials commonly found in residential households and automobiles. These materials may be used in commodity form (e.g. disposable plastic glasses and dishes), expanded form for insulation, impact modified forms such as high impact polystyrene (e.g. appliances and electronics housing), copolymerized with other plastics such as ABS (e.g. toys), or copolymerized with elastomers such as styrene- butadiene rubber (e.g. tires).
- Vinyl polymers also produced considerable amounts of smoke. Again, these materials are used in commodity form (e.g. PVC pipe) or plasticized form (e.g. wiring, siding, resin chairs and tables).
- Average particle sizes ranged from 0.04 to 0.15 microns with wood and insulation generating the smallest particles.
- For a given particle size, synthetic materials will generate approximately 12.5X more particles per mass of consumed material than wood- based materials.
- Combustion of the materials generated asphyxiants, irritants, and airborne carcinogenic species that could be potentially debilitating. The combination and concentrations of gases produced depended on the base chemistry of the material.
- Styrene based materials formed benzene, phenols, and styrene.
- Vinyl compounds formed acid gases (HCl and HCN) and benzene.
- Wood based products formed formaldehyde, formic acid, HCN, and phenols.
- Roofing materials formed sulfur gas compounds such as sulfur dioxide and hydrogen sulfide.
- Collected smoke particulates contained multiple heavy metals including arsenic, cobalt, chromium, lead, and phosphorous, lead, mercury, phthalates and PAHs.
HEALTH IMPLICATIONS
- Multiple asphyxiants (e.g. carbon monoxide, carbon dioxide and hydrogen sulfide), irritants (e.g. ammonia, hydrogen chloride, nitrogen oxides, phenol and sulfur dioxide), allergens (e.g. isocyanates), and chemicals carcinogenic for various tissues (e.g. benzene, chromium, formaldehyde and polycyclic aromatic hydrocarbons) were found in smoke during both suppression and overhaul phases. Carcinogenic chemicals may act topically, following inhalation or following dermal absorption, including from contaminated gear.
- Concentrations of several of these toxicants exceeded OSHA regulatory exposure limits and/or recommended exposure limits from NIOSH or ACGIH.
- Exposures to specific toxicants can produce acute respiratory effects that may result in chronic respiratory disease.
- High levels of ultrafine particles (relative to background levels) were found during both suppression and overhaul phases.
- Exposure to particulate matter has been found to show a positive correlation with increased cardiovascular morbidity and mortality for general population studies.
- The high efficiency of ultrafine particle deposition deep into the lung tissue can result in release of inflammatory mediators into the circulation, causing toxic effects on internal tissues such as the heart. Airborne toxics, such as metals and polycyclic aromatic hydrocarbons, can also be carried by the particles to the pulmonary interstitium, vasculature, and potentially other body tissues, including the cardiovascular and nervous systems and liver.
- Interactions between individual exposure agents could lead to additive or synergistic effects exacerbating adverse health effects.
- Long-term repeated exposure may accelerate cardiovascular mortality and the initiation and progression of atherosclerosis.
- Smoke particles – approx. 2.5 microns in size Red blood cells – approx. 7 microns in size

Left: Smoke particles – approx. 2.5 microns in size: Right: Red blood cells – approx. 7 microns in size.
(Left Image provided by USGS) (Right Image provided by Wikimedia Commons)
THE TOXIC ASSAULT ON THE HUMAN BODY(20)
Toxins enter the human body by several routes including, ingestion, inhalation, injection and absorption. The total toxic load encountered by a body is the sum of all possible routes of entry.
With an exchange surface area approximately that of a tennis court and a very small diffusion distance, the lung is designed for the exchange of gases between inhaled gas and the blood stream. Although the lung is set up this way to facilitate the exchange of oxygen and carbon dioxide as part of normal respiration, it also provides an effective pathway for toxic gases to enter the blood stream. The two most important fire ground toxic gases that utilize this pathway are carbon monoxide (CO) and hydrogen cyanide (HCN), commonly known in the fire service as “The Toxic Twins”. CO works as an asphyxiant by binding hemoglobin 200 times more effectively than oxygen. It eliminates the blood’s ability to deliver oxygen throughout the body. HCN is also an asphyxiant. It attacks the cell’s ability to utilize oxygen and generate energy. Significant exposure to HCN generally results in penalization of respiratory muscle and asphyxiation. More importantly, both HCN and CO are produced in a structural fire. They work synergistically to hurry death by attacking respiration from two sides, oxygen delivery and oxygen use.
 Skin absorption of a toxic substance is far more complicated than inhalation. Many factors affect the rate or even whether or not a substance is absorbed through the skin. The skin can be pictured as a two-layer system. The outer layer, the stratum corneum or epidermis, is a thin layer of dead cells that act as a primary barrier to absorption. Below the epidermis is a much thicker layer of living tissue that contains blood vessels, sweat glands, hair follicles and nerves. Absorption through this system is driven by diffusion alone. When a substance is deposited on, or in contact with skin surface, a concentration gradient is established that drives diffusion. This relationship is described by Fick’s law of diffusion which in essence says, how much of the material reaches the blood stream and contributes to a toxic load is determined by the characteristics of both the compound and the tissue. Fick’s law indicates that the rate of diffusion is determined by several factors including the surface area for diffusion (area of skin contaminated) and the concentration of the contaminant on the skin. In addition, the chemical characteristics of the contaminant are also important. The epidermis is a hydrophobic layer meaning it repels water. Therefore, compounds similar to water will have a difficult time getting through. Organic compounds, like solvents, cross the epidermis more easily. Gases, like HCN and hydrogen sulfide (H2S) move easily across the dermis and, in appropriate concentration, can contribute substantially to a toxic load. Following the movement of a compound from the skin surface to the perfusion rich area of the skin, the amount of blood flow through the skin is another factor which contributes to toxic load.
Skin absorption of a toxic substance is far more complicated than inhalation. Many factors affect the rate or even whether or not a substance is absorbed through the skin. The skin can be pictured as a two-layer system. The outer layer, the stratum corneum or epidermis, is a thin layer of dead cells that act as a primary barrier to absorption. Below the epidermis is a much thicker layer of living tissue that contains blood vessels, sweat glands, hair follicles and nerves. Absorption through this system is driven by diffusion alone. When a substance is deposited on, or in contact with skin surface, a concentration gradient is established that drives diffusion. This relationship is described by Fick’s law of diffusion which in essence says, how much of the material reaches the blood stream and contributes to a toxic load is determined by the characteristics of both the compound and the tissue. Fick’s law indicates that the rate of diffusion is determined by several factors including the surface area for diffusion (area of skin contaminated) and the concentration of the contaminant on the skin. In addition, the chemical characteristics of the contaminant are also important. The epidermis is a hydrophobic layer meaning it repels water. Therefore, compounds similar to water will have a difficult time getting through. Organic compounds, like solvents, cross the epidermis more easily. Gases, like HCN and hydrogen sulfide (H2S) move easily across the dermis and, in appropriate concentration, can contribute substantially to a toxic load. Following the movement of a compound from the skin surface to the perfusion rich area of the skin, the amount of blood flow through the skin is another factor which contributes to toxic load.
Some studies have indicated that absorption of certain chemicals applied to the skin can enter the bloodstream within 26 seconds of contact.
PARTICULATE MATTER AND AIR POLLUTION (21)
Particulate pollution, also called particle pollution or particulate matter (PM), is a mixture of solid particles and liquid droplets in the air. Particles come in many sizes and shapes and can be made up of hundreds of different chemicals. Particulate matter is classified by size. “Fine particles,” or PM2.5, are those smaller than 2.5μm (micrometers, or microns), in diameter, which is about 30 times smaller than the diameter of an average human hair. Coarse particles, or PM10, are between 2.5 and 10μm in diameter. Smaller than PM2.5 are ultrafine particles, PM0.1.
In the Lungs and Bloodstream
 Particles larger than PM10 do not go into the deepest parts of the lungs, and they can be coughed out. Particles smaller than PM10, however, are inhaled into the deepest parts of the lungs, where they become embedded and can cause disease. The smallest ultrafine particles, which are numerous in wood smoke, are so minute they behave like gases, passing through the lungs and directly into the bloodstream. Once in the bloodstream, these ultrafine particles carry toxins around the body and promote inflammation.
Particles larger than PM10 do not go into the deepest parts of the lungs, and they can be coughed out. Particles smaller than PM10, however, are inhaled into the deepest parts of the lungs, where they become embedded and can cause disease. The smallest ultrafine particles, which are numerous in wood smoke, are so minute they behave like gases, passing through the lungs and directly into the bloodstream. Once in the bloodstream, these ultrafine particles carry toxins around the body and promote inflammation.
Bypassing the Blood/Brain Barrier
Ultrafine particles also travel up through the nose and, rather than passing down into the lungs, are delivered directly into the brain and central nervous system via the olfactory nerve, bypassing the body’s protective blood/brain barrier.
Adverse Health Effects and Raised Death Rate
Numerous peer-reviewed studies have described the adverse health effects, including premature death, that are associated with particulate pollution. Effects have been observed at levels as low as 10–20 μg/m3 of PM10, which are levels equal to or below background in many parts of the world. Many studies have shown no evidence of a threshold — an amount under which exposure does not harm health.
Bad for the Heart and Lungs
 Increases in particulate pollution levels can trigger heart attacks, strokes and irregular heart rhythms, especially in those with preexisting heart or lung diseases, and aggravate other lung diseases such as asthma and COPD. Particulate air pollution levels have been significantly associated with hospitalization rates for pneumonia in the elderly. Associations have also been found between small increases in PM2.5 levels and sudden cardiac arrest. A 2013 review in the Lancet found a close and consistent association between short-term exposure to ambient air pollution levels and acute decompensated heart failure and heart failure deaths. The authors estimated that, in the US alone, a mean reduction in PM2.5 of only 3.9 μg/m3 would prevent 7,978 heart failure hospitalizations and save a third of a billion dollars a year.
Increases in particulate pollution levels can trigger heart attacks, strokes and irregular heart rhythms, especially in those with preexisting heart or lung diseases, and aggravate other lung diseases such as asthma and COPD. Particulate air pollution levels have been significantly associated with hospitalization rates for pneumonia in the elderly. Associations have also been found between small increases in PM2.5 levels and sudden cardiac arrest. A 2013 review in the Lancet found a close and consistent association between short-term exposure to ambient air pollution levels and acute decompensated heart failure and heart failure deaths. The authors estimated that, in the US alone, a mean reduction in PM2.5 of only 3.9 μg/m3 would prevent 7,978 heart failure hospitalizations and save a third of a billion dollars a year.
Even Low Levels Increase the Death Rate
A 2015 study of New England Medicare recipients over age 65 determined that the death rate rises for each 10μg/m3 increase in PM2.5, both from short-term and long-term exposure, and even when pollution levels do not exceed US EPA or World Health Organization thresholds. These findings were consistent with those of several other studies that have also found an association between particulate pollution levels and an increase in mortality rate, even at levels that are considered low by regulatory standards.
Like Lead Pollution, There Is No Safe Level
According to Joel Schwartz, senior author of the New England study and professor of environmental epidemiology at Harvard T.H. Chan School of Public Health, this was the first study to examine the effect of airborne soot particles over an entire region.
“The harmful effects from the particles were observed even in areas where concentrations were less than a third of the current standard set by the EPA.” According to Schwartz, “Particulate pollution is like lead pollution; there is no evidence of a safe threshold even at levels far below current standards, including in the rural areas we investigated.”
More recently, Schwartz and other researchers at Harvard looked at data covering 60 million U.S. seniors. This much larger study, which covered approximately 97% of U.S. residents aged 65 and older, similarly found that long-term exposure to PM2.5 increases the risk of premature death, even at levels below current regulatory standards.
Fine Particle Matter Is Officially Recognized as Carcinogenic Linked to Brain Shrinkage and Strokes
Research has shown that long-term exposure to even slightly elevated PM2.5 levels is associated with a .32% smaller total brain volume and a 46% higher risk of silent strokes, even in people who haven’t yet developed dementia or had obvious strokes. It has also been shown that older women living in areas with higher levels of particulate pollution have smaller white matter volumes. Other research has also shown an association between strokes and particulate pollution, especially from “air pollutants related to combustion.” Risk of death from an ischemic stroke is higher when levels of PM2.5 are higher. Even five years after an initial stroke, survival rates are reduced significantly with increased exposure to PM2.5.
Particulate Pollution and Parkinson’s and Alzheimer’s Diseases
Evidence shows that particulate pollution is also a risk factor both in the development and progression of neurodegenerative diseases such as Alzheimer’s and Parkinson’s.
Short-term increases in PM2.5 are associated with an increased risk of hospitalization and an increased risk of death for people with diabetes and, even more so, for people with Parkinson’s disease.
Long-term exposure to elevations in particulate levels is significantly associated with increased first- time hospital admissions for Parkinson’s disease, Alzheimer’s disease and dementia. The risk was seen even at relatively low levels of pollution.
A recent study found that older women residing in places with fine particulate matter exceeding EPA standards had an 81% increased risk of global cognitive decline, and were 92% more likely to develop dementia from any cause, including Alzheimer’s. The risk was even stronger in women who had the APOE4 gene, a genetic variation that increases the risk for Alzheimer’s.
Researchers who study the neuroinflammatory effects of air pollution in young people have declared that exposure to air pollution should be considered a risk factor for Alzheimer’s and Parkinson’s diseases.
More Links to Cognitive Impairment
Another study has also linked fine particulate pollution with worsened cognitive function. It was found that episodic memory is most impaired by exposure to PM2.5. “Episodic memory impairment is one of the core diagnostic criteria used to determine mild cognitive impairment and dementia in older adults, and it has been suggested that impairments in this aspect of memory represent some of the earliest signs of dementia.”
It was noted that particulates can affect the respiratory and cardiovascular systems, which can in turn affect the vascular pathology in the brain. Particulates may even directly damage the brain itself. “Studies of both humans and animals have confirmed that exposure to PM is linked to harmful changes in brain health and functioning.”

Graphic provided by The American Lung Association: http://www.lung.org/our-initiatives/healthy-air/sota/health- risks/
Other studies have also confirmed an association between cognitive decline and long-term exposure to particulate pollution. For example, it was found that exposure to particulate pollution at levels “typically experienced by many individuals in the United States is associated with significantly worse cognitive decline in older women.”
OZONE – REASONS YOU SHOULD NEVER USE AN OZONE GENERATOR TO CLEAN INDOOR AIR (22)
The use of ozone in fire restoration is not a cure-all and it can be very dangerous. After a fire, it is all too common to hear “industry experts” advocate for the use of ozone as the silver bullet to completely sanitize the air and remove all particulate matter. Unfortunately, much of the material that supports the use of ozone makes claims and draws conclusions without substantiation or sound science. There are even some vendors which suggest that their devices have been approved by the federal government, despite the fact that there is not one agency within the federal government which has approved ozone generators for use in occupied spaces. The EPA published several documents which highlight the risks and dangers of ozone and why ozone generators should be avoided.
The reliance on ozone alone to remove or neutralize all contaminants is similar to a hospital filled with patients with all sorts of ailments. The same medicine that may work for one will not work for everyone else and many may have adverse reactions or end up not being treated at all.
Why is Ozone Dangerous?
Ozone is a tiny molecule composed of three oxygen atoms. It is highly reactive which makes it an unstable and potentially toxic gas. Ground-level ozone is considered to be a major component of smog which plagues larger cities during the summertime and has been tied to a variety of potential health risks.
Health Effects of Ozone & Particle Pollution
The EPA has reported there is a variety of health effects associated with high levels of ozone. Ozone is the most widespread pollutant in the U.S. It is also one of the most dangerous pollutants.
Exposure to ozone may include decreased lung function, throat irritation, severe asthma symptoms, cough, chest pain, shortness of breath, irritation of lung tissue, and the higher sensitivity to respiratory infection. They went on to note that there were additional risk factors which can perpetuate the side effects of ozone such as undertaking activities which raise breathing rates (such as exercising indoors), certain pre-existing lung diseases, and greater duration of exposure.
4 Reasons Why You Should Avoid Air Purifiers that Produce Ozone
- Ozone Generators May Not Work at All
Some manufacturers suggest that ozone will render nearly every chemical contaminant in the home harmless by producing a chemical reaction. This is incredibly misleading because a thorough review of scientific research has shown that in order for many of the dangerous chemicals found indoors to be eliminated the chemical reaction process may take months or even years. Other studies have also noted that ozone cannot effectively remove carbon monoxide. If used at concentrations that do not exceed public health standards, ozone applied to indoor air pollution does not effectively remove viruses, mold, bacteria, or other pollutants. - The Chemical Reaction Can Be Dangerous
Even if ozone generators were proven to be effective at eliminating these chemicals, there are certain side effects everyone must be aware of. Many of the chemicals ozone reacts to results in a variety of harmful by-products. For example, when ozone was mixed with chemicals from new carpet in a laboratory setting, the ozone created a variety of dangerous organic chemicals in the air. - Ozone Generators Do Not Remove Particulates
A third factor to consider when looking at ozone generators is that they do not remove particulates from the air. This includes the particles which are primarily responsible for allergic reactions or respiratory ailments. To combat this, some ozone generators include an ionizer which disperses negatively charged ions into the air. In recent analysis’s, this process was found to be less competent in the removal of air-borne molecules of dust, smoke, pollen, and mold spores than HEPA filters and electrostatic precipitators. - It Is Impossible to Predict Exposure Levels
The EPA notes that it is increasingly difficult to determine the actual concentration of ozone produced by an ozone generator because so many different factors come into play. Concentrations will be higher if more powerful devices are used in smaller spaces. Additional factors which affect concentration levels include how many materials and furnishings are in the room to react with ozone, the level of outdoor air ventilation, and the proximity of a person to the ozone generating device.
HEPA Filters: The Safer & More Effective Solution. Choosing a HEPA or Ultra Low Penetration Air (ULPA) filter is a significantly safer and more effective solution to removing particulates than an ozone generator. Instead of releasing dangerous ozone, a HEPA or ULPA filter traps indoor air pollutants rather than trying to create a chemical reaction with them. In many cases, this type of filter is often combined with other technologies, such as activated carbon, to provide even better results. Utilizing a pre-filter and activated carbon, air purifiers can remove solid, chemical, and gaseous pollutants from the air and dramatically improve indoor air quality.
Toxic Byproducts Created With Ozone
Ozone reacts with certain chemicals that can produce toxic byproducts. Here are five:
- Ozone reacts with contaminants to create nitrogen dioxide. (23)
Nitrogen dioxide is corrosive to the skin and the respiratory tract and is a key ingredient in smog. Inhalation of the gas or the vapor may cause lung oedema. Exposure far above the occupational exposure limit may result in death. The effects may be delayed. (24) - Ozone reacts with terpenes to create formaldehyde.
Terpenes are organic compounds and major components of resin, and of turpentine produced by conifer trees (pines, cedars, spruces, redwoods, etc.) Reactions of ozone and terpenes lead to the production of carbonyls such as formaldehyde and acetaldehyde, organic acids, hydrogen peroxide, secondary organic aerosols and hydroxyl radicals. Produced hydroxyl radicals would chain-react with VOC’s or carbonyl compounds in indoor environments, resulting in the generation of additional oxidation products. Information about many of the individual byproducts during ozone oxidation of terpenes is limited. Additionally, the mixture of oxidation products appears to have significant irritant properties. Acetaldehyde and formaldehyde were not decomposed by ozone.(25) - Ozone reactions can create formic acid.
Formic acid is a medium strong acid that reacts violently with oxidants and attacks many plastics and metals. It can be absorbed into the body by inhalation of its vapor, through the skin and by ingestion. The substance is very corrosive to the eyes, the skin and the respiratory tract. Corrosive on ingestion. Inhalation of the vapor may cause lung oedema and may cause effects on the energy metabolism, resulting in acidosis. (26)Given the complexity of the chemical reactions that occur, additional research is needed to more completely understand the complex interactions of indoor chemicals in the presence of ozone.Even with high levels of ozone, contaminants embedded in porous material may not be affected at all. (27) - Ozone reacts with water vapor and creates hydrogen peroxide.
Hydrogen peroxide was observed when water vapor was present. The ‘water effect’ is the result of a direct reaction of water vapor with the Criegee biradical (the main intermediate in reactions of ozone with alkenes).(28) Although it resembles oxygen in many respects, ozone is much more reactive; hence, it is an extremely powerful oxidizing agent, particularly useful in converting olefins into aldehydes, ketones, or carboxylic acids.(29) - A byproduct of ozonation is Methyl Bromide (Bromomethane)
Byproducts of ozonation that have been identified include bromate, bromomethanes, brominated acetic acids, brominated acetonitriles and ketones. (30)Methyl bromide is used as a fumigant and pesticide and is highly toxic. Studies in humans indicate that the lung may be severely injured by the acute (short-term) inhalation of methyl bromide. Acute and chronic (long-term) inhalation of methyl bromide can lead to neurological effects in humans. Neurological effects have also been reported in animals. Degenerative and proliferative lesions in the nasal cavity developed in rats chronically exposed to methyl bromide by inhalation.Acute Effects of Methyl Bromide:
Studies in humans indicate that the lung may be most severely injured by the acute inhalation exposure of methyl bromide. Breathing high concentrations of methyl bromide may cause pulmonary edema, impairing respiratory function. Acute exposure by inhalation of methyl bromide frequently leads to neurological effects in humans. Symptoms of acute exposure in humans include headaches, dizziness, fainting, apathy, weakness, confusion, speech impairment, visual effects, numbness, twitching, and tremors; in severe cases paralysis and convulsions are possible. Acute exposure may produce delayed effects. Symptoms may improve without treatment in less serious cases. Methyl bromide is irritating to the eyes, skin, and mucous membranes of the upper respiratory tract. Dermal exposure to methyl bromide can cause itching, redness, and blisters in humans. Kidney damage has been observed in humans who have inhaled high levels of methyl bromide. Injury to the heart has been observed in mice and rats exposed to high concentrations of methyl bromide by inhalation. Tests involving acute exposure of rats and mice have demonstrated methyl bromide to have high acute toxicity from inhalation and oral exposure. (31)
The Importance of VOC Testing Prior to Fire Damage Restoration Activities
Restoration contractors, insurance companies, investigators, content cleaning companies, and any employer that sends their employees into a fire damaged home or building are required by federal law to protect their workers from hazardous atmospheres, including those created after structure fires.
OSHA Regulation 1910.134(d)(1)(iii)
Before employees enter potentially harmful atmospheres, the employer must identify and evaluate the respiratory hazards. The employer shall identify and evaluate the respiratory hazard(s) in the workplace; this evaluation shall include a reasonable estimate of employee exposures to respiratory hazard(s) and an identification of the contaminant’s chemical state and physical form. This requires air sampling and analysis. Where the employer cannot identify or reasonably estimate the employee exposure, the employer shall consider the atmosphere to be immediately dangerous to life or health (IDLH).
IDLH means an atmosphere that poses an immediate threat to life, would cause irreversible adverse health effects, or would impair an individual’s ability to escape from a dangerous atmosphere.” (32)
This would include the highly toxic VOC’s, chemicals, and particulates generated by the variety of building materials and products that may have burned in the fire. Without question, fire VOC testing is needed to identify health hazards that are associated with chemical compounds present in a post-fire environment.
In addition, employers must characterize the nature and magnitude of employee exposures to respiratory hazards before selecting respiratory protection equipment.
When must an employer conduct an exposure assessment?
When you expose your employees to a respiratory hazard and/or require them to wear respirators. Examples of when you should consider assessments may include but are not limited to:
- When OSHA has a substance specific standard (e.g., lead, methylene chloride).
- When employees notice symptoms (e.g., irritation, odor) or complain of respiratory health effects.
- When the workplace contains visible emissions (e.g., fumes, dust, aerosols).
What is the identity and nature of the airborne contaminant?
Specific characteristics of the airborne hazard must be established in order to select an appropriate respirator.
- Is the airborne contaminant a particulate (dust, fumes, mist, aerosol) or a gas/vapor?
- Is the airborne contaminant a chemical and are material safety data sheets available?
- Is the airborne contaminant a biological (bacteria, mold, spores, fungi, virus)?
- Are there any mandatory or recommended occupational exposure levels for the contaminant?(33)
CONCLUSION:
The information compiled in this paper provides compelling evidence that fire restoration practitioners insurance adjusters, and consumers need to consider when addressing smoke, VOC’s, and particulate matter generated by structure fires. Anyone entering a fire or smoke damaged environment needs to consider the potential health risks and take necessary precautions to protect their health and safety. People who have their properties or belongings damaged by fire or smoke also need to be informed of the health hazards they may be exposed to long after the restoration process is completed if proper restorative measures aren’t taken.
Currently, the EPA has over 85,000 chemicals registered in its inventory of substances that fall under the Toxic Substances Control Act and approximately 2,000 new chemicals are introduced each year. (34) The Chemical Abstracts Service is the world’s authority on chemical information and it has over 142 million registered organic and inorganic substances in its registry.(35) These chemicals are combined in more than 7 million mixture formulations that are found in homes and buildings across the U.S. (36) and the majority of the chemicals currently in commercial use haven’t been evaluated.(37) This means we have no idea how dangerous some of these chemicals or their byproducts could be, especially in a post-fire environment.
Every fire has its own DNA and the methods to restore fire or smoke damaged buildings and contents varies. The types and quantities of materials and products that combusted, their chemical reactions, intensity of heat and other factors make each post-fire environment unique. Equally unique are the measures needing to be taken to remove odors and contaminants to achieve a successful restoration.
Assessing the uniqueness of each fire restoration project and performing preliminary particulate and VOC testing are the first crucial steps in determining a restoration plan. Restoration contractors should avoid introducing deodorizers, thermal fogs, aerosols, or other chemicals into fire or smoke damaged environments, without knowing first whether potentially reactive chemicals and VOC’s might generate toxic byproducts. Without a thorough analysis of contaminants (fire VOC testing, particulate samples, lift samples, etc.) to determine what chemicals, gases, or contaminants are present, restorers will have no idea what they may be dealing with. This can expose workers, property owners, and occupants to a myriad of potentially hazardous toxins and health risks.
Historically, it has been a common practice for restoration contractors to use deodorizers as a means to restore fire damaged buildings, soft goods, clothing, and textiles. However, the use of deodorizers or odor counteractants often does nothing more than mask or camouflage hazardous contaminants, leaving people exposed to hazardous toxins that can later be inhaled, ingested, or absorbed by the skin. Toxic smoke particulates are invisible and many are odorless and although you may not be able to smell smoke odor or see evidence of soot, doesn’t mean the air, surfaces, fabrics, or materials aren’t contaminated. The only way to determine whether a smoke contaminated environment or material has been effectively restored is by performing a comprehensive smoke particulate and VOC clearance test or fabric analysis after the cleaning and deodorization process has been completed.
This process is very similar in concept to mold remediation or asbestos abatement, where an industrial hygienist performs sampling before remediation commences, surveys the spore or fiber count, and generates a remediation protocol. Then, once the remediation is completed, an air clearance test is used to verify whether the work was successful in removing the contaminants.
Today, textiles exposed to certain contaminants such as asbestos, lead, mold, or sewage are usually discarded. However, when clothes, soft goods, or other textiles are exposed to smoke related contaminants, they are often sent to be treated and cleaned. Without scientific analysis, how can consumers be assured that toxic particulate matter has actually been removed or if toxic particulates might be trapped in the material fiber mesh?
Science and technology have advanced to the point now where we have more knowledge and understanding about the chemistry of fire and smoke and the proper ways to restore buildings and materials impacted by them. Careful consideration needs to be given to not only the visible damages of a fire, but also the indoor air quality and environmental hazards caused by the release of hazardous chemicals and toxins.
The following points summarize a few of the key findings of the research compiled in this paper:
- Residual smoke, soot, chemicals, VOC’s, and microscopic particulates generated from structure fires are hazardous to human health and exposure can cause severe injury, damage the DNA of individuals and their progeny(38), and even cause death.
- Toxic particulate matter can enter the body through the lungs or by contact with the skin.
- Toxic particulate matter can adversely affect the health of everyone. Those at the greatest risk of injury are infants, children, the elderly, and those with weakened respiratory systems or cardiac ailments.
- Particulate pollution is like lead pollution; there is no evidence of a 100% safe threshold of exposure.
- Ozone and Hydroxyl can produce hazardous byproducts and are not proven to be 100% effective to remove all toxic chemicals or particulate matter from surfaces or the air.
- Sealing or encapsulating exposed surfaces or applying liquid deodorizers does not address toxic particulate matter suspended in the air, soot, or VOC’s. Relying on these methods alone will most likely leave occupants exposed to hazards associated with toxic particulates and odor reoccurrence.
- Toxic particulate matter must be properly remediated prior to the return of occupants who may live or work in or around the affected areas.
- Proper personal protective equipment should be worn by anyone entering an environment affected by fire smoke. This would include outer coveralls such as Tyvek® suits, a fit tested respirator with P-100 type filters designed for vapors or a supplied air or powered air-purifying respirator, gloves, boots, etc.
STEPS TO ENSURE A RESTORED INDOOR AIR ENVIRONMENT
Exposure to toxic smoke particulates and VOC’s can pose a greater health risk than that of toxic mold, asbestos, or lead-based paint dust exposure. In order to restore the indoor air quality after a fire, similar procedures and protocols used in the mold, asbestos, and lead abatement industry should be employed. These steps should be taken to properly clean and restore the indoor air quality, primarily by removing the particulates rather than relying solely on treating, deodorizing, or masking them. Steps would include, but are not limited to: Having a preliminary air sample test performed to determine what types and concentrations of chemicals and particulates are present. This is important, so chemicals used in the cleaning process don’t accidently interact with the chemicals or gases present, which may produce more toxic byproducts. Then setting up containments, wearing proper personal protective equipment, running negative air filtration with HEPA or ULPA filters, HEPA vacuuming surfaces, deodorizing, and encapsulation of exposed surfaces, etc. Once the cleaning process is completed, an independent environmental testing company should be hired to provide testing that includes, but is not limited to:
- Surface dust wipe samples to test surfaces for combustion byproduct particulate matter including soot, char & ash.
- Surface dust wipe samples to test for the presence of dioxins and metals including lithium, chromium, lead, mercury, etc.
- Air samples to test for VOC’s and smoke particulate matter associated with burned materials, paints, glues, plastics, synthetic materials, etc.
- Air clearance sampling to verify that the air has been properly cleaned of toxic particulate matter. An air clearance should be achieved prior to project completion and reentry of occupants.
The ultimate goal of a successful restoration is to eliminate the presence of fire related contaminants or at a minimum, bring the concentration levels well below the National Institute for Occupational Safety and Health (NIOSH) permissible exposure limits (PELs) or the lowest limits mandated by any other federal, state, or local governing agencies. For a list of chemicals and their exposure limits provided by NIOSH or OSHA visit: https://www.cdc.gov/niosh/docs/2005-149/default.html or https://www.osha.gov/dsg/annotated-pels/
For more information on testing for toxic smoke particulates and VOC’s, or air quality clearance testing, contact Bruce Rosenblatt with Rarefied Air Environmental at 619-888-4840.
SOURCES:
-
- U.S. Department of Health and Human Services – “How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease, A Report of the Surgeon General” 2010
- United States Environmental Protection Agency – “How Smoke from Fires Can Affect Your Health” https://www.epa.gov/pm-pollution/how-smoke-fires-can-affect-your-health
- American Institute for Conservation of historic and Artistic Works – “The Hidden Hazards of Fire Soot” by: Dawn Bolstad-Johnson http://www.conservation-us.org/docs/default-source/periodicals/2010-09-sept-aicnews.pdf?sfvrsn=6
- Industrial Hygiene – “What is Soot and Why is it Dangerous?” http://blog.cashins.com/blog-0/bid/191511/Industrial-Hygiene-What-is-Soot-and-Why-is-it-Dangerous Posted by Zachary Keefe
- Science Direct – “Chemical Agents” by: Ian Greaves and Paul Hunt http://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/diphosgene
- U.S. National Library of Medicine National Institutes of Health “Enhanced TCDD degradation by Fenton’s reagent preoxidation” by: J. Hazard Mater https://www.ncbi.nlm.nih.gov/pubmed/10794914
- Medical Effects: “Dioxin and PCB’s From Wood Burning” [Science, Vol. 266 Oct. 21, 1994,T.J. Nestrick and L.L. Lamparski, Anal. Chem. 54, 2292 (1982)]. http://burningissues.org/car-www/medical_effects/dioxin.htm
- World Health Organization “Dioxins and their effects on human health” http://www.who.int/mediacentre/factsheets/fs225/en/
- A Guide to Living Plasticless – dioxins http://plasticisrubbish.com/2008/06/03/dioxins-poisons-contamination/
- World Health Organization- “Dioxins and their effects on human health” http://www.who.int/mediacentre/factsheets/fs225/en/
- U.S. Environmental Protection Agency – “Dioxins Produced by Backyard Burning” https://www.epa.gov/dioxin/dioxins-produced-backyard-burning and World Health Organization “Dioxins and their effects on human health” http://www.who.int/mediacentre/factsheets/fs225/en/
- Medical Effects: “Dioxin and PCB’s From Wood Burning” http://burningissues.org/car-www/medical_effects/dioxin.htm
- World Health Organization – “Dioxins and their effects on Human Health” http://www.who.int/mediacentre/factsheets/fs225/en/
- U.S. National Library of Medicine National Institutes of Health “An Overview of the Effects of Dioxins and Dioxin-like Compounds on Vertebrates, as Documented in Human and Ecological Epidemiology” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788749/
- The Aspen Institute https://www.aspeninstitute.org/programs/agent-orange-in-vietnam-program/health-effects/
- “Why is Dioxin So Dangerous?” By: Don Fitz, Gateway Green Alliance http://www.greens.org/s-r/078/07-06.html
- Columbia Universiy – “Substance and Perceptions of Environmental Impacts of Dioxin Emissions” by: Panagiotis G. Deriziotis http://www.seas.columbia.edu/earth/wtert/sofos/Deriziotis_thesis_final.pdf
- Science Direct – “Toxicokenetics and Mechanism of Toxicity” http://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/asphyxiant-gas
- “Firefighter Exposure to Smoke Particulates” http://www.commandsafety.com/2010/11/09/firefighter-exposure-to-smoke-particulates/
- Fire Smoke Coalition – Atmospheric Monitoring: the Comprehensive Guide – “Fire Smoke Gases: Where are they, and what will they do to you?” Page 15 “The Toxic Assault on the Human Body” http://www.raesystems.com/sites/default/files/content/resources/ebook_atmospheric-monitoring.pdf
- Doctors and Scientists Against Wood Smoke Pollution – “Particulate Matter and Air Pollution” https://woodsmokepollution.org/particulate-pollution.html
- Allergy and Air -Ozone– “4 Reasons You Should Never Use An Ozone Generator to Clean Indoor Air” https://learn.allergyandair.com/ozone-generators/
- U.S. National Library of Medicine National Institutes of Health – “Toxicity, Ozone” by Terrell J. Swanson;
Jennifer Chapman https://www.ncbi.nlm.nih.gov/books/NBK430751/ - The National Institute for Occupational Safety & Health (NIOSH) Nitrogen Dioxide – International Chemical Safety Cards https://www.cdc.gov/niosh/npg/npgd0454.html
- International Journal of Environmental research and Public Health – “Measurement of Secondary Products During Oxidation Reactions of Terpenes and Ozone Based on the PTR-MS Analysis: Effects of Coexistent Carbonyl Compounds” by: Yusuke Ishizuka, Masahiro Tokumura, Atsushi Mizukoshi, Miyuki Noguchi, and Yukio Yanagisawa https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2996213/
- The National Institute for Occupational Safety & Health (NIOSH) Formic Acid – International Chemical Safety Cards https://www.cdc.gov/niosh/npg/npgd0296.html
- U.S. Environmental Protection Agency Indoor Air Quality – “Ozone Generators that are sold as Air Cleaners” https://www.epa.gov/indoor-air-quality-iaq/ozone-generators-are-sold-air-cleaners
- International Journal of Science “Production of Hydrogen Peroxide in Forest Air By Reaction of Ozone with Terpenes” by: Karl H. Becker, Klaus J. Brockmann & Joseph Bechara and “What Is Ozone” by: Envron Environmental, Ltd. http://www.nature.com/articles/346256a0 and https://envronozone.com/science/ozone_science.htm
- Encyclopedia Britannica – “Ozone – Chemical Allotrope” https://www.britannica.com/science/ozone
- World Health Organization – WHO seminar pack for drinking-water quality http://www.who.int/water_sanitation_health/dwq/S04.pdf
- U.S. Environmental Protection Agency – Methyl Bromide (Bromomethane) https://www.epa.gov/sites/production/files/2016-09/documents/methyl-bromide.pdf
- U.S. Occupational Safety and Health Administration Regulation 1910.134(d)(1)(iii) https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134
- U.S. Occupational Safety and Health Administration – Exposure Assessment https://www.osha.gov/SLTC/etools/respiratory/change_schedule_exposure.html
- PBS – “It could take centuries for EPA to test all the unregulated chemicals under a new landmark bill” By: Mark Scialla: https://www.pbs.org/newshour/science/it-could-take-centuries-for-epa-to-test-all-the-unregulated-chemicals-under-a-new-landmark-bill
- Chemical Abstracts Service https://cen.acs.org/acs-news/programs/CAS-reaches-150-millionth-substance/97/web/2019/05
- Characterization of Fire Investigators Exposure During Fire Scene Examination By: Dennis L. Rogers – DuPage County Arson Task Force (page 19)
- Australian Government Federal Register of Legislation – Safety, Rehabilitation and Compensation Amendment (Fair Protection for Firefighters) Act 2011 https://www.aph.gov.au/Parliamentary_Business/Committees/Senate/Education_Employment_and_Workplace_Relations/Completed_inquiries/2010-13/firefighters/report/c02
- U.S. National Library of Medicine National Institutes of Health “Origin and Health Impacts of Emissions of Toxic By-Products and Fine Particles from Combustion and Thermal Treatment of Hazardous Wastes and Materials” By: Stephania A. Cormier,Slawo Lomnicki, Wayne Backes, and Barry Dellinger https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1480527/
Some of the information contained in this document was provided by the following agencies:

DISCLAIMER:
This paper is distributed as a public service for informational purposes only. While reasonable efforts were made to ensure the completeness and accuracy of its contents when published, no warranties or guarantees are made with respect to the completeness or accuracy of the information and opinions stated herein. The information and opinions stated herein may not be applicable to or suitable for every individual or situation and constitute the opinions of the Author and the sources of the information sited. Neither the Author nor Heritage Publishing & Communications, Ltd., shall be responsible to any user of the information for any injury, loss or damage of any kind or nature whatsoever that may be sustained as a consequence of the use and application of any information or opinions presented. In no event shall the Author nor Heritage Publishing & Communications, Ltd., be liable for any action taken or not taken by any person in reliance, directly or indirectly, upon the information and opinions provided herein. This publication is provided with the understanding that the Author, is not engaged in rendering legal advice and no legal opinions are provided by the Author. If legal or other professional advice or expert assistance is required, the services of a competent professional should be obtained.
All persons and entities using the information and opinions provided herein do so at their own risk and they hereby waive any and all claims against the Author and Heritage Publishing & Communications, Ltd. Such waiver includes any and all claims arising in contract or tort, and all forms of equitable relief and damages including without limitation compensatory, general, special, and consequential damages.
Without limiting any other disclaimer provided herein, under no circumstances shall the Author be liable for any injury, loss, or damage of any kind or nature whatsoever. Information in this newsletter relates to a subject that changes periodically due to changes in industry practices, science, and technology. All users of this paper acknowledge this disclaimer and agree to the limitations of liability stated above.
Do not use this information if you do not agree with this disclaimer and its limitations of liability as reasonable. If any portion of this disclaimer is found to be unenforceable under applicable law, the remainder of the disclaimer will remain enforceable.
ABOUT SEAN SCOTT:
 Mr. Scott is a licensed general contractor in the State of California who has spent over 39 years in the construction and restoration industry. As a second-generation fire and flood restoration contractor, he has been involved with literally thousands of property damage claims ranging from commercial and residential floods and fires, smoke claims, mold contaminations, subsidence and earthquake claims, explosions, vehicular collisions, and many other types of property damaging incidents. Throughout his career, Sean has worked with all the major insurance carriers that underwrite residential and commercial policies and has worked directly with claims adjusters, independent adjusters, third party administrators, public adjusters, and attorneys. Sean is also the author of two books, The Red Guide to Recovery – Resource Handbook for Disaster Survivors and Secrets of the Insurance Game and the co-author of a third book titled The Native Family Disaster Preparedness Handbook.
Mr. Scott is a licensed general contractor in the State of California who has spent over 39 years in the construction and restoration industry. As a second-generation fire and flood restoration contractor, he has been involved with literally thousands of property damage claims ranging from commercial and residential floods and fires, smoke claims, mold contaminations, subsidence and earthquake claims, explosions, vehicular collisions, and many other types of property damaging incidents. Throughout his career, Sean has worked with all the major insurance carriers that underwrite residential and commercial policies and has worked directly with claims adjusters, independent adjusters, third party administrators, public adjusters, and attorneys. Sean is also the author of two books, The Red Guide to Recovery – Resource Handbook for Disaster Survivors and Secrets of the Insurance Game and the co-author of a third book titled The Native Family Disaster Preparedness Handbook.
Sean has devoted his life to assisting individuals and families rebuild their homes, businesses, and lives and has witnessed first-hand the physical, emotional, and financial challenges people face once the first responders leave the scene. Since 2009, Sean’s award-winning book The Red Guide to Recovery has been adopted by fire departments, emergency management agencies, and relief organizations across the U.S.
Sean now uses his time and expertise to help people navigate the recovery process, speak on recovery and restoration topics, and consult with those in the restoration industry who need guidance to be more successful. He also provides expert witness testimony, estimating services on property damage claims, insurance claim appraisal and umpire services, construction defect investigation, and training.
For more information on disaster restoration and recovery, The Red Guide to Recovery – Resource Handbook for Disaster Survivors and Secrets of The Insurance Game both provide a wealth of insight and information on the recovery process.

For more information, contact: Sean Scott
Office: 858-453-6767
Cell: 858-349-2262
Email: Sean@TheRedGuideToRecovery.com
Website: TheRedGuideToRecovery.com
©Copyright Heritage Publishing & Communications, Ltd. All Rights Reserved 2018